1. Introduction: The “Wicked” Problem of the Evidence-Practice Gap
As clinical leaders, we face a persistent challenge: the gap between high-level research and the actual treatment of patients in our clinics. Traditionally, we have viewed implementation as a linear process, yet we continue to struggle with improving consistent outcomes. We must recognize that wound care is a wicked problem—an environment characterized by synergistic, multiple interactions where “nothing stands still while we intervene.”
Evidence alone does not solve clinical problems. To drive real change, we must move beyond the passive “dissemination” of data and embrace knowledge mobilization. This requires a strategic shift toward narrative engagement and co-production, ensuring that scientific rigor is integrated into the “Life-World” of our clinicians and patients.
2. Understanding the Ecosystem: Health Systems as Complex Adaptive Systems
To lead innovation, we must stop treating our hospitals as machines that can be perfectly controlled through top-down mandates. Instead, we must manage them as Complex Adaptive Systems (CAS). In a CAS, change is emergent and constant; it occurs naturally as individuals acquire new information and adapt their behaviors.
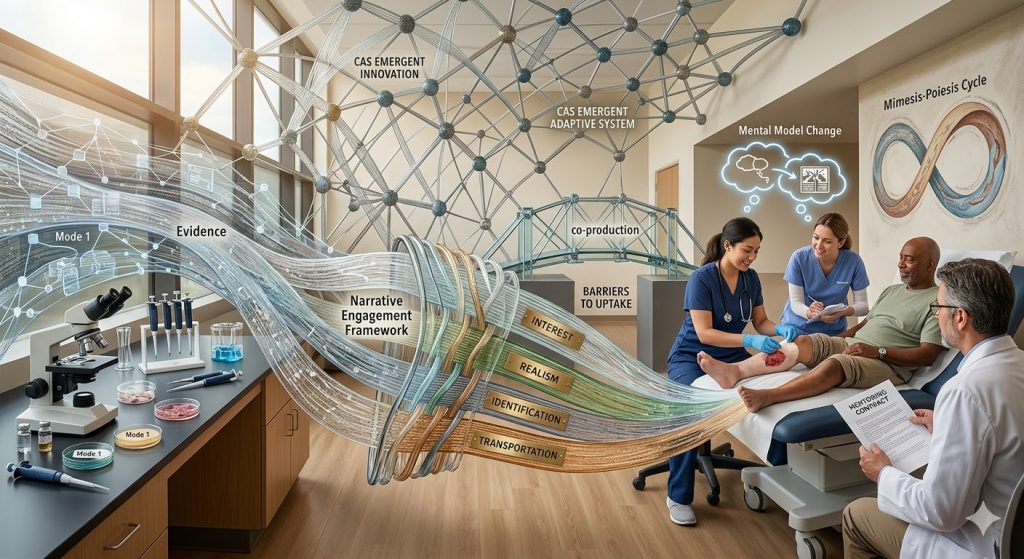
This perspective shifts our focus from “Mode 1” research (curiosity-driven science generated in academic isolation) to “Mode 2” research, which is collaborative, problem-based, and co-produced by those on the front lines.
Strategic Implementation Matrix: Control vs. Complexity
| Feature | Control-Based Approach | Complexity-Informed Approach |
| Logic | Linear: Assumes a one-way flow from researcher to user. | Iterative: Knowledge is co-produced through ongoing interaction. |
| Execution | Predictive: Relies on pre-planning and rigid protocols. | Emergent: Solutions emerge through trial and local adaptation. |
| Innovation | Pilot-Focused: Tests “fixes” in controlled, static settings. | Prototype-Focused: Refines innovations through constant feedback. |
| Staff Mindset | Compliance-driven: Focuses on following the rulebook. | Learning-driven: Focuses on adapting to patient needs. |
3. The Science of Knowledge Translation (KT) and Mobilization
In the framework of Knowledge-to-Action (KTA), evidence is not a static object but a process shaped by professional and political contexts. We utilize the Narrative Engagement Framework (NEF) to bridge the gap. According to Exemplification Theory, narratives act as powerful exemplars—vivid surrogates for direct personal experience that help clinicians process complex information.
Narratives facilitate education by influencing “mental models”—the internal scripts clinicians use to guide decision-making. These stories serve three critical functions:
- Mental Model Building: Developing new scripts for clinicians facing unfamiliar wound etiologies.
- Mental Model Change: “Re-storying” experiences for staff whose current practices are anchored in outdated or ineffective protocols.
- Mental Model Maintenance: Reinforcing best practices that already align with our clinical goals.
To enhance Behavioral Modeling, we utilize “near-peer” scenarios. By using slightly more experienced residents or nurses in training modules, we leverage higher “messenger-based credibility,” allowing juniors to observe skill application and conflict resolution in a relatable context.
4. Navigating Barriers to Evidence Uptake
Identifying barriers is only the first step; we must understand how these constraints interact unpredictably:
- Structural Barriers: Perverse incentives often reward volume over value, while tight budgets frame research as a “competitor” to care rather than its engine.
- Leadership Failures: Traditional “Command and Control” styles stifle the inter-organisational and inter-sectoral cooperation required for systemic change.
- Epistemological Gaps: There is a fundamental disconnect between Mode 1 academic priorities (focused on generalizable, de-identified data) and the Life-World of the patient and caregiver (rooted in unique, individual experiences of suffering).
5. Strategic Bridging: Co-Production and Narrative Mimesis
Bridging the gap requires the “co-production” of knowledge, where researchers and clinicians frame questions together to ensure academic expertise is immediately useful to the clinical flow.
Practical Mobilization Models
- Researcher-in-Residence: We embed academics directly into clinical teams. This researcher moves beyond observation to actively negotiate between scientific evidence and the practicalities of a busy wound clinic.
- The Mimesis-Poiesis Cycle: Drawing from Ricoeur’s phenomenology, we view patient care through the lens of mimesis (creative imitation of experience) and poiesis (the re-creation or “rebirth” of the narrator). By “re-storying” a patient’s journey, we help move them from “mute suffering” to being an active agent in their own healing.
The Elements of Narrative Engagement
To make clinical guidelines “sticky,” we design training around the four elements of the NEF:
- Interest: The intensity of attention paid to the clinical message.
- Realism: The perceived authenticity and believability of the scenario.
- Identification: The degree to which the clinician feels “at one” with the characters.
- Transportation: The cognitive and emotional absorption into the story, allowing the clinician to envision new possibilities for care.
6. Becoming Champions: Leading the Interprofessional Specialty
Wound care excellence requires coordinated management. As Directors, we must transition our teams into institutional champions of Evidence-Based Practice (EBP) using this strategic checklist:
- Mentorship Contracts: We must go beyond informal pairings and use formal “Mentoring Contracts.” These align expectations not just on milestones, but on Personal Conduct and Interpersonal Relations, ensuring psychosocial support and professional trust (Source: Huskins).
- The “Central Place” Strategy: We must advocate for dedicated outpatient wound clinics. While this model “exposes” costs that are typically “dispersed” and hidden across a hospital, we justify the investment through a significant reduction of inpatient days and re-admission rates—a primary financial driver for hospital administrators.
- Social Proliferation: We leverage the natural spread of ideas. Effective narratives “proliferate” through social networks, where peer discussion reinforces desirable behaviors more effectively than a standard lecture.
- Evaluation for Learning: We are moving away from only tracking wound closure rates. We must implement Process Measures to evaluate the health of our mobilization efforts:
- Frequency and results of evidence-based discussions.
- Clinician and patient satisfaction with the relationship.
- Alignment between mentor and scholar expectations.
7. Conclusion: A Call to Action for Clinical Emergence
To heal wounds effectively, we must work with the complexity of our health systems. We must “re-story” the relationship between research and the clinical “Life-World,” moving toward a model where evidence is co-produced and human-centric.
Critical Takeaways for Clinical Innovation:
- Adopt a Complexity Mindset: Recognize that healthcare is a CAS; we must allow solutions to emerge through iterative prototyping rather than rigid command-and-control mandates.
- Leverage Narrative Power: Use the NEF (Interest, Realism, Identification, and Transportation) to shift mental models and foster social proliferation of best practices through near-peer exemplars.
- Institutionalize Co-Production: Implement “Researcher-in-Residence” models and “Mentoring Contracts” that explicitly align expectations on personal conduct to build a high-trust, evidence-driven culture.